________________
Annexure-1
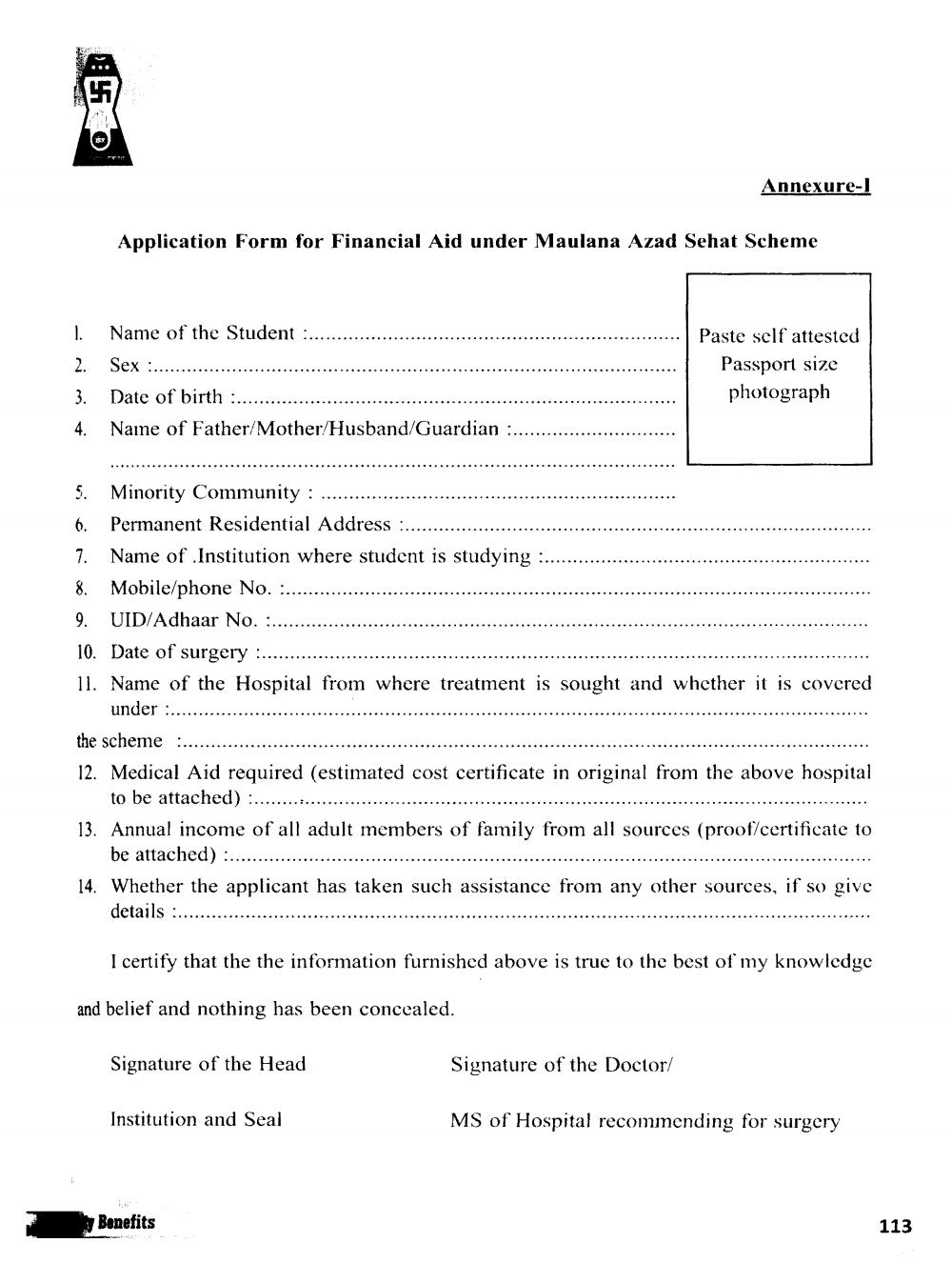
Application Form for Financial Aid under Maulana Azad Sehat Scheme
1. Name of the Student :..... 2. Sex :............ 3. Date of birth :........... 4. Naine of Father/
Mother/Husband/Guardian ..........
Paste self attested
Passport size photograph
..............
5. Minority Community :.... 6. Permanent Residential Address :..... .......... 7. Name of Institution where student is studying 8. Mobile/phone No. :......... 9. UID/Adhaar No. :...... 10. Date of surgery ....... 11. Name of the Hospital from where treatment is sought and whether it is covered
under .............. the scheme .................................... 12. Medical Aid required (estimated cost certificate in original from the above hospital
to be attached) .......... 13. Annual income of all adult members of family from all sources (proof/certificate to
be attached) ........ 14. Whether the applicant has taken such assistance from any other sources, if so give
details
.....
I certify that the the information furnished above is true to the best of my knowledge
and belief and nothing has been concealed.
Signature of the Head
Signature of the Doctor/
Institution and Seal
MS of Hospital recommending for surgery
Benefits
113